Chronic idiopathic constipation (CIC) is an ongoing condition without any known cause or identified underlying illness. Constipation is a condition that can be defined as a state of unsatisfactory defecation, with characteristic features of infrequent stools and difficulty in passing stools, or both. Eight million people in the US seek medical care for constipation every year, and one million are hospitalized. It is likely that many people who have CIC do not report the condition to their doctors because they are embarrassed or do not see it as a major problem requiring medical care.
CIC and Irritable Bowel Syndrome both present as chronic constipation, and are distinct from acute constipation. Acute constipation usually has an organic cause, such as medication or a medical condition, while chronic constipation usually does not, although medication can sometimes play a role. The term idiopathic means that the disorder arises spontaneously, without any known cause. Chronic idiopathic constipation, therefore, is a type of chronic constipation that has no obvious cause. It is a form of functional constipation.
CIC is characterized by infrequent stools which are often difficult to pass. It typically affects women and older adults. The typical symptom of this condition is passing fewer than 3 bowel movements per week for more than 6 months.
To diagnose CIC, a physician usually excludes all other causes of constipation. The treatment options are limited but include dietary changes and physical exercise.
Symptoms
Infrequent bowel movements and difficulty passing stool, are the most common symptoms. If you experience any of the symptoms listed below more than 25% of the time for six months or more, you may need to be assessed for CIC.
- Straining
- Hard stools
- A feeling of incomplete evacuation, i.e. a sensation of stool remaining in the bowel after defecating
- A feeling of blockage in the anus or rectum
- Use of manual maneuvers, such as using the hands, to facilitate defecation
In addition, a major symptom is having fewer than three bowel movements a week.
Good to know: Irritable Bowel Syndrome shares some symptoms with chronic idiopathic constipation, but people with IBS report pain and bloating more often than people with CIC, and report that their symptoms improve after defecation. This is not the case with CIC. People with CIC almost never experience diarrhea without using laxatives.1 They also experience normal loose stools only rarely. For more information, see this resource on on Irritable Bowel Syndrome. If you are experiencing uncomfortable symptoms, you can do a symptom assessment using the free Ada app at any time.
There are several gastroenterological symptoms which indicate that chronic constipation may have a serious medical condition as its underlying cause, rather than being idiopathic. These include:
Distended abdomen/severe bloating
- Vomiting
- Blood in the stool
- Hematochezia5
- Unintended weight loss
- Anemia
- Severe constipation of recent onset
- Rapid worsening of constipation
- Family history of colon or rectal cancer
These symptoms are more likely to indicate a serious underlying condition in people who are over 50 years of age at the time of symptoms first appearing.
Good to know: Constipation is a possible symptom of colorectal cancer, a common gastroenterological cancer that usually affects people who are older than 60 years of age. It is associated with Crohn’s disease and ulcerative colitis. For more information, see this resource on colorectal cancer.
Causes
CIC is most commonly seen in women and older adults. The causes of chronic idiopathic constipation are largely unknown. However, possible causes include a reduction in fluid and fiber intake in the diet, changes in water balance, and changes in contractility of the colon.
There are several different forms of CIC:
- Normal transit constipation, where the stool may be harder than normal and therefore more difficult to pass, but moves through the colon at a normal speed
- Slow transit constipation, where stools move through the colon more slowly than usual
- Disorders of defecation or evacuation
Disorders of defecation or evacuation include:
- Rectocele, a condition where the wall of the rectum bulges into the wall of the vagina inside the body and forms a pouch
- Rectal prolapse, a condition where the rectum protrudes through the anus and becomes visible outside the body
- Dyssynergic dysfunction
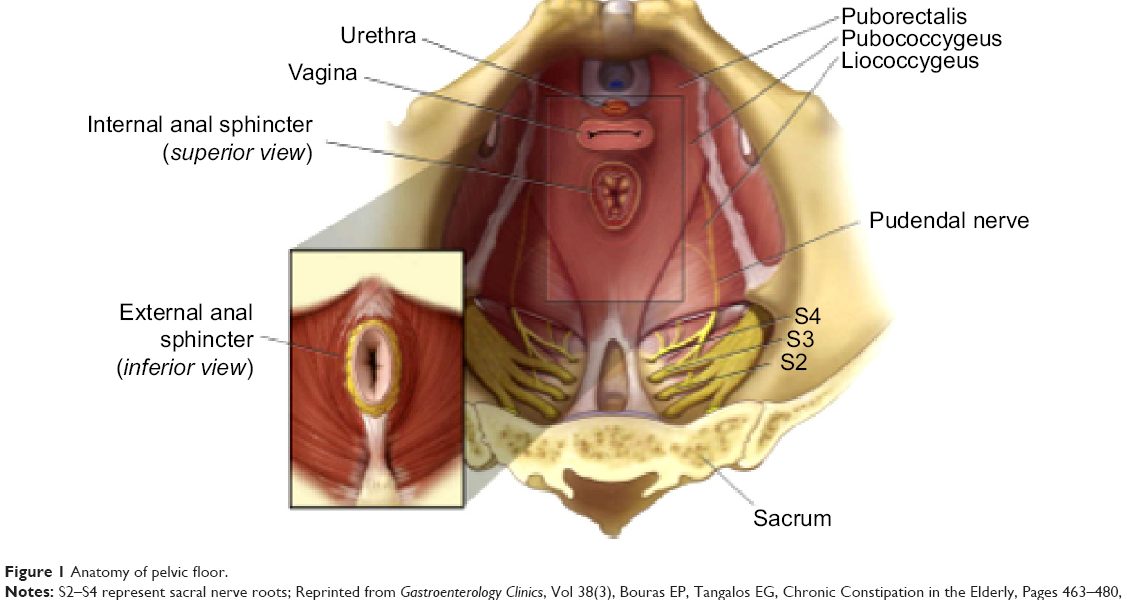
Dyssynergic dysfunction arises from problematic co-ordination of the various muscles and sphincters that control defecation. Defecation requires the muscles involved to coordinate the creation of increasing pressure inside the rectum, followed by relaxation of the internal and external anal sphincters and relaxation of the perineal muscles. This requires the coordination of the pelvic floor muscles, abdominal muscles, and the muscles in the rectum.
If these structures do not work together, defecation becomes difficult. People experiencing dyssynergic dysfunction often report a feeling of obstruction and incomplete evacuation. Complications of dyssynergic dysfunction include rectocele, anal fissure and rectal prolapse.
In some cases, chronic constipation may be caused by certain medications, such as:
- Antihistamines
- Antipsychotic medications
- Antispasmodic medications
- Opioids
- General anesthetics
- Antiparkinsonian drugs
Good to know: Medication-related constipation may be chronic (long-lasting) or acute (short-term), and may improve if use of the medication that is causing it is stopped.
Diagnosis
The diagnosis is usually based on the symptoms that a person is experiencing and on conducting a physical examination. To confirm the diagnosis, all other causes of constipation – for example a medical condition, or medication – should be excluded.
Doctors who treat constipation are often specialists in gastroenterology. There are various international gastroenterological criteria that help doctors to determine whether CIC, rather than IBS, is present.
Some tests that may be done to aid diagnosis include:
- Colonoscopy, in which an endoscopic camera is inserted into the colon, used to identify structural problems. See this resource for more information on preparing for a colonoscopy.
- Blood tests to check for infection and other disorders. See this resource for more information on blood test results.
Colonoscopy is used conservatively. MRI scans are also used sometimes.
Good to know: If the person with CIC does not meet the criteria for being at high risk of colorectal cancer, doctors will usually be conservative about ordering diagnostic tests and instead rely on taking a history from the affected person and evaluating their symptoms. Tests such as manometry, motility capsules, Sitz markers and scintigraphy are generally rarely used.
Treatment
As it is not possible to determine the cause of CIC, the treatment options tend to be limited. Dietary changes, like increasing dietary fiber and water intake are usually helpful, as is doing regular physical exercise. However, diet, fluid intake and exercise are not uniformly effective, and some people with CIC may be recommended to use:
- Fibre supplements such as psyllium, calcium polycarbophil, inulin and maltodextrin
- Osmotic laxatives such as polyethylene glycol or lactulose
- Stimulant laxatives such as bisacodyl, glycerol or sodium picosulfate
Laxatives can help with softening stool and improving regularity of bowel movements. Fibre supplements have a similar effect.
People who do not find that laxatives provide enough relief from the symptoms of CIC, or for whom laxatives are not recommended, may find serotonin agonists, such as prucalopride or velusetrag, useful.
However, the main medications that are recommended when laxatives do not work or cannot be used are lubiprostone (a fatty acid) and linaclotide (an oligo-peptide agonist). These medications work by increasing the amount of chloride that is secreted into the gut, which increases the amount of fluid in the gut, which in turn stimulates bowel movements. One side effect of linaclotide is diarrhea. Otherwise, both drugs are very effective for CIC.
The list of some Chronic idiopathic constipation medicine: