
Olaparib (Lynparza®) is available as both a tablet and a capsule and a surprisingly common assumption among patients, caregivers, and even some dispensing pharmacists is that the two are equivalent. They are not.
Switching between olaparib tablets and capsules without medical guidance can lead to meaningful dosing errors. The approved doses differ between the two formulations, the bioavailability profiles are not the same, and the approved clinical indications have evolved differently across markets. Treating them as simple substitutes creates real risk.
This article explains exactly how the two formulations differ, why the doses are not interchangeable, what each formulation is approved to treat, and what prescribers, pharmacists, and patients need to verify before dispensing or taking either form.
What Is Olaparib and Why Does Formulation Matter?
Olaparib is a PARP (poly ADP-ribose polymerase) inhibitor used in the treatment of several cancers — primarily ovarian, breast, pancreatic, and prostate cancers in patients with BRCA mutations or other defects in homologous recombination repair.
It exists in two distinct pharmaceutical formulations: a hard capsule (50 mg) and a film-coated tablet (100 mg and 150 mg). These are not different packaging for the same product. They were developed at different times, studied in separate clinical trials, and approved at different doses because their pharmacokinetic behaviour differs.
Understanding which formulation is prescribed and why is essential for safe, effective treatment.
Olaparib Tablets vs Capsules — At a Glance
| Feature | Olaparib Tablet | Olaparib Capsule |
|---|---|---|
| Available strengths | 100 mg, 150 mg (film-coated) | 50 mg (hard capsule) |
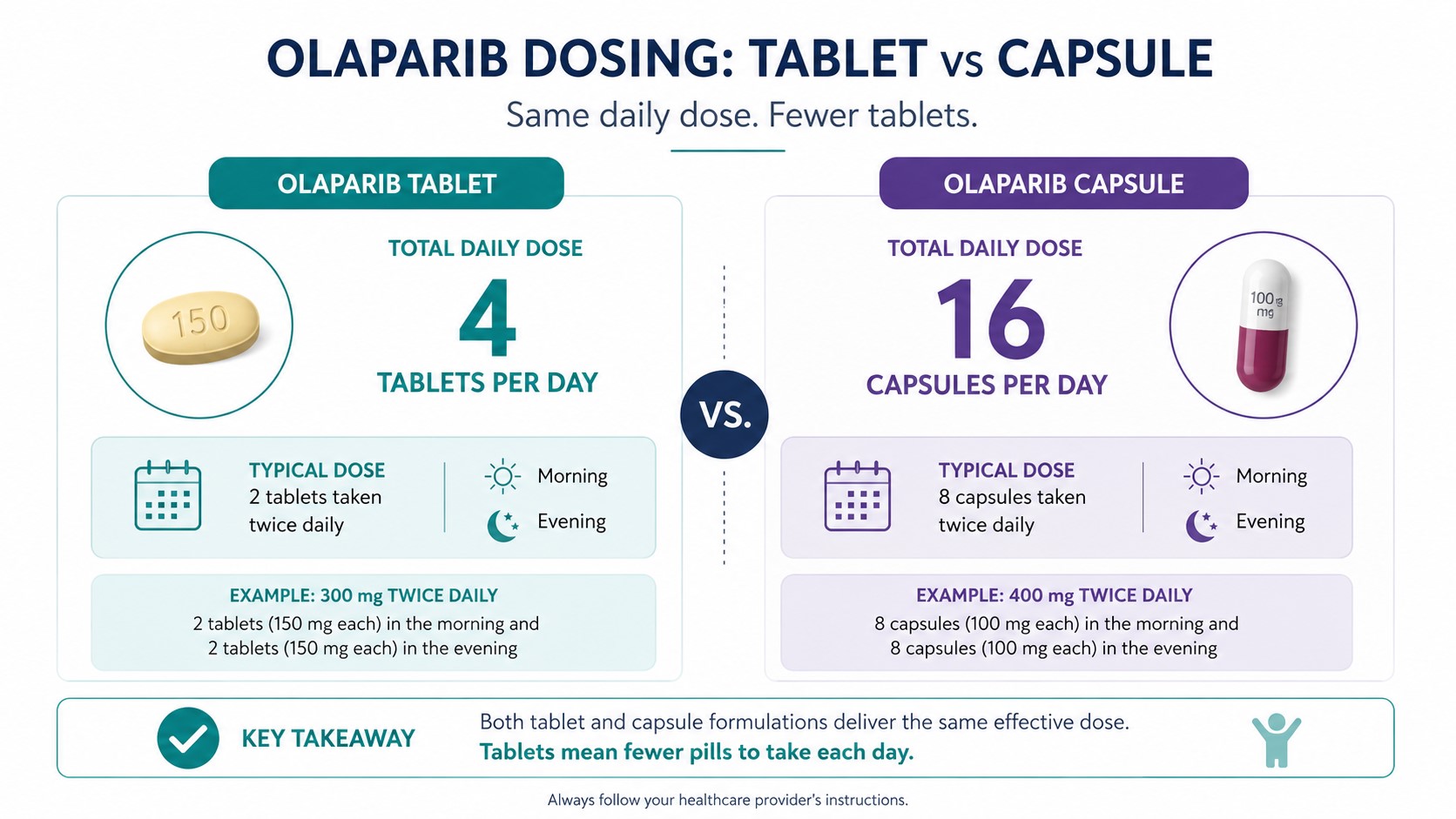
| Standard adult dose | 300 mg twice daily (two 150 mg tablets) | 400 mg twice daily (eight 50 mg capsules) |
| Daily pill count | 4 tablets | 16 capsules |
| Bioavailability | Higher (ASD melt-extrusion formulation) | Lower (crystalline olaparib in lipid base) |
| Interchangeable? | No | No |
| Storage (typical) | Room temperature (per current SmPC) | Refrigerated at 2°C–8°C; may be kept at room temperature (≤30°C) for up to 3 months |
| Food interaction | Can be taken with or without food | Avoid high-fat meals close to dosing (check current prescribing information) |
| Current preference | Now the standard formulation in most markets | Being phased out in many countries |
Always confirm current storage and administration requirements against the approved prescribing information for your market.
Tablet Formulation (Film-Coated)
Olaparib tablets are available in two strengths: 100 mg and 150 mg. The standard recommended adult dose is 300 mg twice daily, typically administered as two 150 mg tablets taken in the morning and two in the evening — four tablets per day in total.
The tablet was developed using an amorphous solid dispersion (ASD) melt-extrusion technology, which significantly improves how olaparib is absorbed in the gastrointestinal tract compared to the original capsule. This improved bioavailability is what allows the effective dose to be lower despite delivering comparable or greater systemic exposure.
The tablet formulation has been studied and approved across a range of tumour types, including BRCA-mutated ovarian, fallopian tube, and primary peritoneal cancers; germline BRCA-mutated HER2-negative metastatic breast cancer; BRCA-mutated metastatic pancreatic cancer; and BRCA-mutated or homologous recombination repair-deficient metastatic prostate cancer. Approved indications vary by regulatory authority and market — always verify locally.
Capsule Formulation (Hard Capsule)
Olaparib capsules contain 50 mg of olaparib per capsule in a hard gelatin shell with a lipid-based excipient (lauroyl macrogol glycerides). The standard approved dose is 400 mg twice daily, which requires a patient to take eight capsules per dose — sixteen capsules per day.
This high pill burden was a significant drawback of the capsule formulation from the patient experience perspective and was one of the primary motivations for developing the tablet. The capsule relies on a lipid vehicle to aid dissolution, which is why storage requirements are stricter and why food interactions must be managed carefully.
In most regulated markets — including the EU, UK, and US — the capsule formulation has been largely superseded by the tablet. However, it may still be in use in some countries based on regulatory approval timelines or supply availability. Healthcare providers in Bangladesh and South Asia should verify current local availability and approval status.
Are Olaparib Tablets and Capsules Bioequivalent?
No. Olaparib tablets and capsules are not bioequivalent, even at matched milligram doses.
The tablet formulation uses a melt-extrusion ASD technology that significantly increases the rate and extent of olaparib absorption. Clinical pharmacokinetic studies showed that at doses above 100 mg, exposure to the capsule formulation increased less than proportionally with dose, while exposure to the tablet formulation increased approximately proportionally. This non-linear behaviour of the capsule is why a higher capsule dose (400 mg) was needed in clinical trials, even though the resulting systemic exposure is still lower than that achieved by the 300 mg tablet dose.
Specifically, population pharmacokinetic analyses from the FDA prescribing information showed that steady-state exposure (AUC) following 300 mg tablet twice daily was approximately 77% higher than that following 400 mg capsule twice daily. This is not a marginal difference — it reflects fundamentally different absorption profiles between the two formulations.
The ASD tablet formulation was estimated to enhance olaparib bioavailability by approximately 2.65-fold compared to the capsule, which is what enabled the dose reduction from 400 mg to 300 mg while maintaining or exceeding therapeutic exposure.
This means that if a patient receives olaparib capsules at a dose of 300 mg (six capsules twice daily) instead of the approved 400 mg, they will receive meaningfully less drug exposure than intended. Conversely, prescribing the capsule dose (400 mg) in place of the tablet dose without adjustment would not simply “replace” the tablet — the bioavailability difference changes what the patient actually receives.
The two formulations cannot be substituted for each other without a prescriber explicitly reviewing and adjusting the dose.
Approved Indications — Does the Formulation Affect What Olaparib Can Treat?
This is where the formulation distinction matters beyond pharmacokinetics.
Because the tablet and capsule formulations were studied in separate clinical trials at different times, their regulatory approval histories differ. The capsule formulation was studied in earlier-phase trials that established olaparib’s clinical proof of concept. The tablet was subsequently studied in the pivotal Phase III trials — including SOLO-2 in platinum-sensitive recurrent ovarian cancer and OlympiAD in BRCA-mutated metastatic breast cancer — that formed the basis for regulatory approval in most major markets.
As a result, in markets like the US and EU, the tablet formulation now holds the primary approved indications for olaparib. The capsule’s regulatory footprint may be narrower or absent for certain indications depending on the country and approval timeline.
For prescribers and pharmacists in Bangladesh: The DGDA (Directorate General of Drug Administration) governs local approvals. The regulatory status of each olaparib formulation in Bangladesh — and which indications are approved locally — should be verified directly with the DGDA or through a licensed pharmaceutical supplier. Do not assume that indications approved by the FDA or EMA automatically apply to locally registered products.
Dosing Differences and How to Avoid Medication Errors
Understanding the dose difference is not simply a matter of knowing the numbers. It requires understanding that the dose of each formulation was established through separate clinical development programs, and that the numbers are not exchangeable on a ratio basis.
| Formulation | Standard Dose | Capsules/Tablets Per Dose | Daily Pill Count |
|---|---|---|---|
| Olaparib Tablet | 300 mg twice daily | 2 × 150 mg tablets | 4 tablets |
| Olaparib Capsule | 400 mg twice daily | 8 × 50 mg capsules | 16 capsules |
It is not correct to simply take six capsules (300 mg) instead of the approved eight (400 mg) and assume equivalence with the tablet dose. The systemic exposures produced are different because of the bioavailability difference between formulations.
Equally, if a patient is switched from the tablet to the capsule — for example, due to supply constraints — the dose cannot simply be “translated” by matching the milligram number. A prescriber must explicitly review the formulation change and prescribe the appropriate dose for the new formulation.
For drug interactions involving CYP3A4 modulators, dose adjustments are formulation-specific. When olaparib is co-administered with a strong CYP3A4 inhibitor, the tablet dose should be reduced to 100 mg twice daily, while the capsule dose should be reduced to 150 mg twice daily. These are different numbers and cannot be applied interchangeably.
Common Dosing Mistakes to Avoid
- Assuming the tablet and capsule doses are equivalent milligram-for-milligram. They are not. 300 mg tablet ≠ 300 mg capsule in terms of exposure.
- Switching formulations without prescriber review. Any change from tablet to capsule or vice versa requires explicit prescribing guidance and dose verification.
- Dispensing the wrong formulation due to labelling confusion. Both products carry the Lynparza® brand name. Confirm the formulation (tablet or capsule) and strength before dispensing.
- Crushing or splitting olaparib tablets. Film-coated tablets should be swallowed whole. Crushing may alter drug release and absorption.
- Incorrect storage of capsules. Capsules require refrigeration unless specific conditions for room-temperature storage are met. Dispensing capsules that have been incorrectly stored may affect product integrity.
- Applying CYP3A4 dose-adjustment rules from one formulation to the other. Drug interaction dose reductions are formulation-specific and cannot be transferred between tablet and capsule.
- Assuming locally unapproved indications apply. Always check which indications have been approved for which formulation in the relevant local market.
Storage, Handling, and Patient Practical Considerations
Beyond dosing, the two formulations differ in ways that affect day-to-day patient experience and pharmacy management.
Storage: Olaparib capsules require refrigeration at 2°C to 8°C. They may be kept at room temperature not exceeding 30°C for up to three months, but must not be frozen or exposed to temperatures above 40°C. This creates a specific cold-chain requirement during distribution and pharmacy storage. Olaparib tablets are stored at controlled room temperature — a meaningful logistical simplification for patients and dispensing pharmacies, particularly in regions with variable refrigeration access.
Pill burden: Sixteen capsules per day versus four tablets per day is not a trivial difference. Research on cancer treatment adherence consistently shows that pill burden is a predictor of non-adherence. A patient managing fatigue, nausea, or other treatment-related side effects faces a meaningfully different daily task depending on which formulation they are prescribed. For most patients, the tablet offers a substantially more manageable regimen.
Tablet integrity: Olaparib tablets should not be crushed, split, or chewed. Patients with swallowing difficulties should discuss alternatives with their clinical team rather than modifying the tablet.
Administration with food: Administration recommendations may differ between formulations. Patients should follow the specific guidance in the prescribing information for their formulation rather than applying guidance from one to the other.
Which Olaparib Formulation Is Available in Bangladesh?
The availability of specific olaparib formulations in Bangladesh depends on DGDA registration status, local distributor networks, and supply agreements with originator or licensed manufacturers.
Patients, oncologists, and procurement teams in Bangladesh should not assume that both formulations are available, or that what is available is the formulation most recently studied in clinical trials. Supply and registration can differ from global market norms.
Medicine for World (https://mfw.com.bd/) works with healthcare providers and patients across Bangladesh to source and verify the availability of oncology medicines including olaparib. If you are a prescriber or patient looking to confirm which olaparib formulation is currently available and appropriately registered in Bangladesh, contact the Medicine for World pharmaceutical team directly for guidance before prescribing or purchasing.
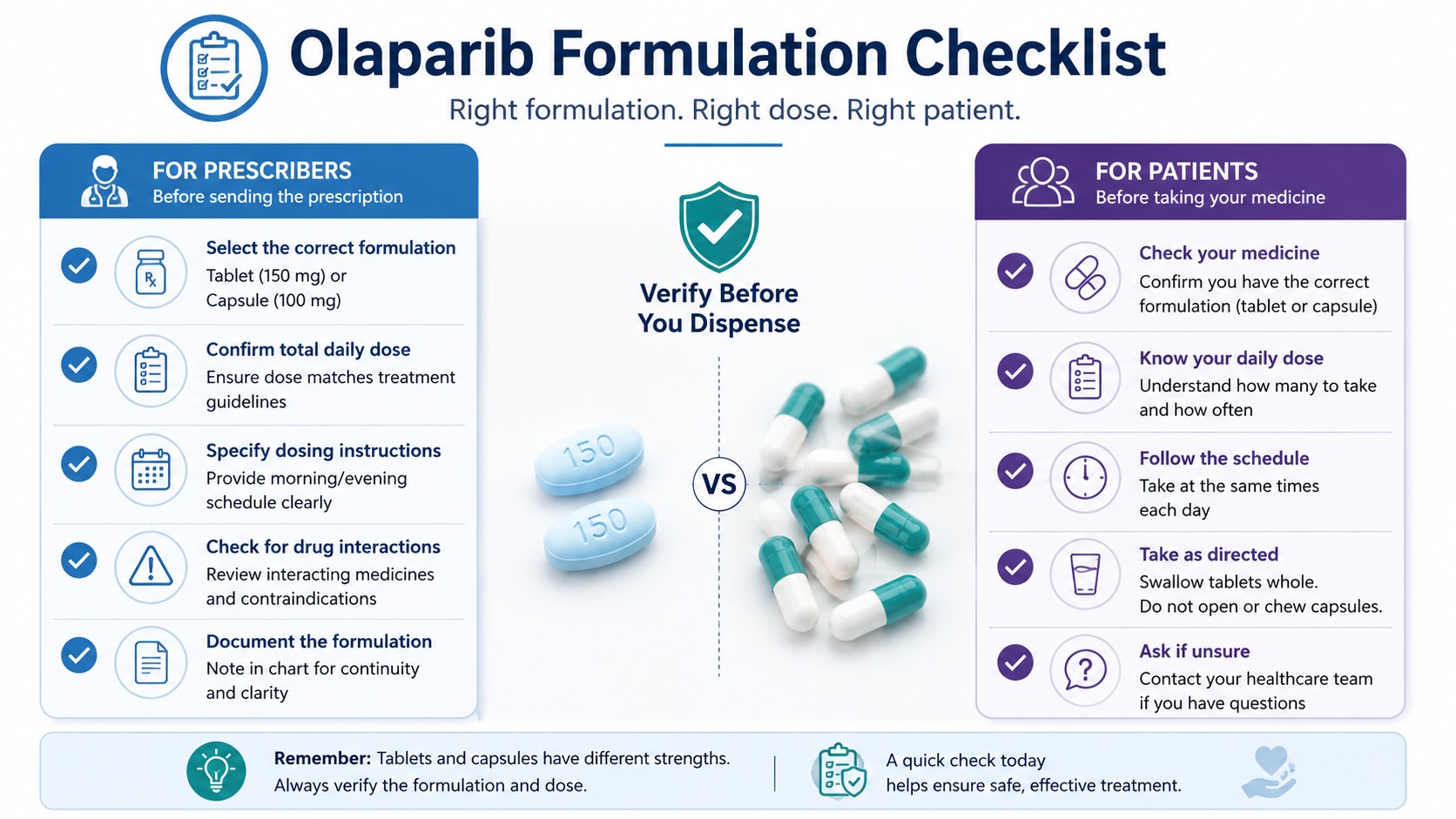
Practical Checklist for Prescribers and Patients
Use this checklist before dispensing, prescribing, or taking olaparib:
For prescribers and pharmacists:
- Confirm the exact formulation being prescribed: tablet or capsule
- Confirm the correct dose for that specific formulation (300 mg bd for tablet; 400 mg bd for capsule unless adjusted)
- Verify that the formulation and indication are locally approved by DGDA or the relevant regulatory authority
- If the patient is on a CYP3A4 inhibitor or inducer, apply the dose-adjustment guidance for the correct formulation — do not cross-apply between tablet and capsule
- Counsel the patient on correct storage requirements for the formulation dispensed
- Do not substitute one formulation for the other without explicitly reviewing and adjusting the dose
For patients:
- Know whether you have been prescribed tablets or capsules — check your prescription and the pack carefully
- Do not take a different formulation than what was prescribed without first speaking to your oncologist or pharmacist
- Store your medication according to the instructions on the pack — tablets and capsules may have different requirements
- Take each dose as prescribed; do not adjust the number of tablets or capsules without medical guidance
- If your supply changes formulation (e.g. due to availability), contact your prescriber before taking the new product
Key Takeaways
- Olaparib tablets and olaparib capsules both contain the same active ingredient but are not interchangeable due to differences in bioavailability.
- The standard tablet dose is 300 mg twice daily (four tablets per day); the standard capsule dose is 400 mg twice daily (sixteen capsules per day).
- The tablet formulation delivers approximately 77% higher AUC at steady state compared to the capsule at its approved dose, due to an improved melt-extrusion formulation technology.
- Approved indications may differ between formulations depending on the country and local regulatory authority — always verify with DGDA or your prescribing information.
- Any switch between formulations must be reviewed by a prescriber, and the dose must be explicitly confirmed for the new formulation.
- The tablet is now the preferred and predominant formulation in most major markets; the capsule has been largely phased out but may still be in circulation in some regions.
Frequently Asked Questions
Are olaparib tablets and capsules the same drug?
Yes — both contain olaparib as the active pharmaceutical ingredient. However, they are different formulations with different approved doses, different bioavailability profiles, and different storage requirements. They are not interchangeable. The tablet formulation is now the standard form in most markets, offering a lower pill burden and improved absorption compared to the capsule.
What is the dose difference between olaparib tablets and capsules?
The standard adult dose for olaparib tablets is 300 mg twice daily — taken as two 150 mg tablets per dose, four tablets per day. For olaparib capsules, the standard dose is 400 mg twice daily — eight 50 mg capsules per dose, sixteen capsules per day. These doses are not milligram-equivalent and cannot be directly substituted. The tablet produces higher systemic drug exposure despite the lower milligram dose, due to its improved bioavailability.
Can I switch from olaparib capsules to tablets without consulting my doctor?
No. Switching formulations without medical guidance carries a real risk of dosing error. Because the bioavailability profiles differ, a new dose must be confirmed for the new formulation by your prescribing oncologist. In clinical studies, switching was managed under protocol. If your formulation changes due to supply constraints or any other reason, contact your prescriber before taking the new product.
Which olaparib formulation is approved for use in Bangladesh?
Regulatory approval status in Bangladesh is governed by the DGDA and can change over time. Patients and healthcare providers should verify current approved formulations and indications locally. Medicine for World (https://mfw.com.bd/) can assist with verifying availability and sourcing of registered olaparib products in Bangladesh.
Why does olaparib exist in both tablet and capsule form?
The capsule was the original formulation used in early clinical trials when olaparib was first being developed. Because olaparib has poor water solubility, the initial capsule relied on a lipid-based excipient to aid absorption — but this approach had limitations at higher doses, requiring patients to take sixteen capsules per day. A tablet using melt-extrusion technology was subsequently developed to improve bioavailability and significantly reduce pill burden. The tablet became the preferred clinical formulation following positive Phase III trial results and now holds the primary regulatory approvals in most major markets.
Conclusion
The difference between olaparib tablets and capsules is not cosmetic. It is clinical, pharmacokinetic, and regulatory. The two formulations are not interchangeable, the doses are not equivalent on a milligram basis, and approved indications may differ depending on where you are in the world. Treating them as simple alternatives risks meaningful dosing errors that could affect both the safety and efficacy of treatment.
For oncologists, pharmacists, and patients, the key principle is straightforward: always confirm the exact formulation prescribed, apply the dose that was approved for that specific formulation, and never switch between the two without explicit prescriber review.
For verified information on olaparib formulation availability in Bangladesh, reach out to the Medicine for World team at mfw.com.bd — a trusted resource for oncology medicines and pharmaceutical guidance in Bangladesh.

