Disclaimer: This article is for informational purposes only. Always consult a qualified oncologist or clinical pharmacist before making any treatment decisions. This content has been prepared for educational use and does not constitute medical advice.
TL;DR — Key Differences at a Glance
- Olaparib (Lynparza): The most broadly approved PARP inhibitor – covers ovarian, breast, prostate, and pancreatic cancers. Best studied in BRCA-mutated patients.
- Niraparib (Zejula): Approved for ovarian cancer maintenance regardless of BRCA status. Does not require a biomarker test to prescribe.
- Rucaparib (Rubraca): Voluntarily withdrawn from the US market for prostate cancer in 2022; limited current use. Most relevant for ovarian cancer in BRCA-mutated patients.
- Bottom line: Olaparib has the widest indications. Niraparib is the go-to for maintenance therapy without biomarker selection. Rucaparib’s role has significantly narrowed.
Introduction
Choosing a cancer treatment is never simple. When an oncologist mentions PARP inhibitors, patients and caregivers often face a wall of unfamiliar names – Olaparib, Niraparib, Rucaparib and very little clarity on what makes each one different.
These three drugs belong to the same drug class and share a mechanism of action. But they differ in their approved uses, dosing schedules, side effect profiles, and which patients benefit most. Getting this wrong means either missing an effective therapy or taking on unnecessary risks.
This article breaks down each drug clearly – what it does, who it is for, how it compares to the others, and how oncologists actually choose between them. At Medicine for World, we believe patients deserve evidence-based information they can discuss confidently with their care team.
What Is a PARP Inhibitor and How Does It Work?
The Role of PARP in DNA Repair
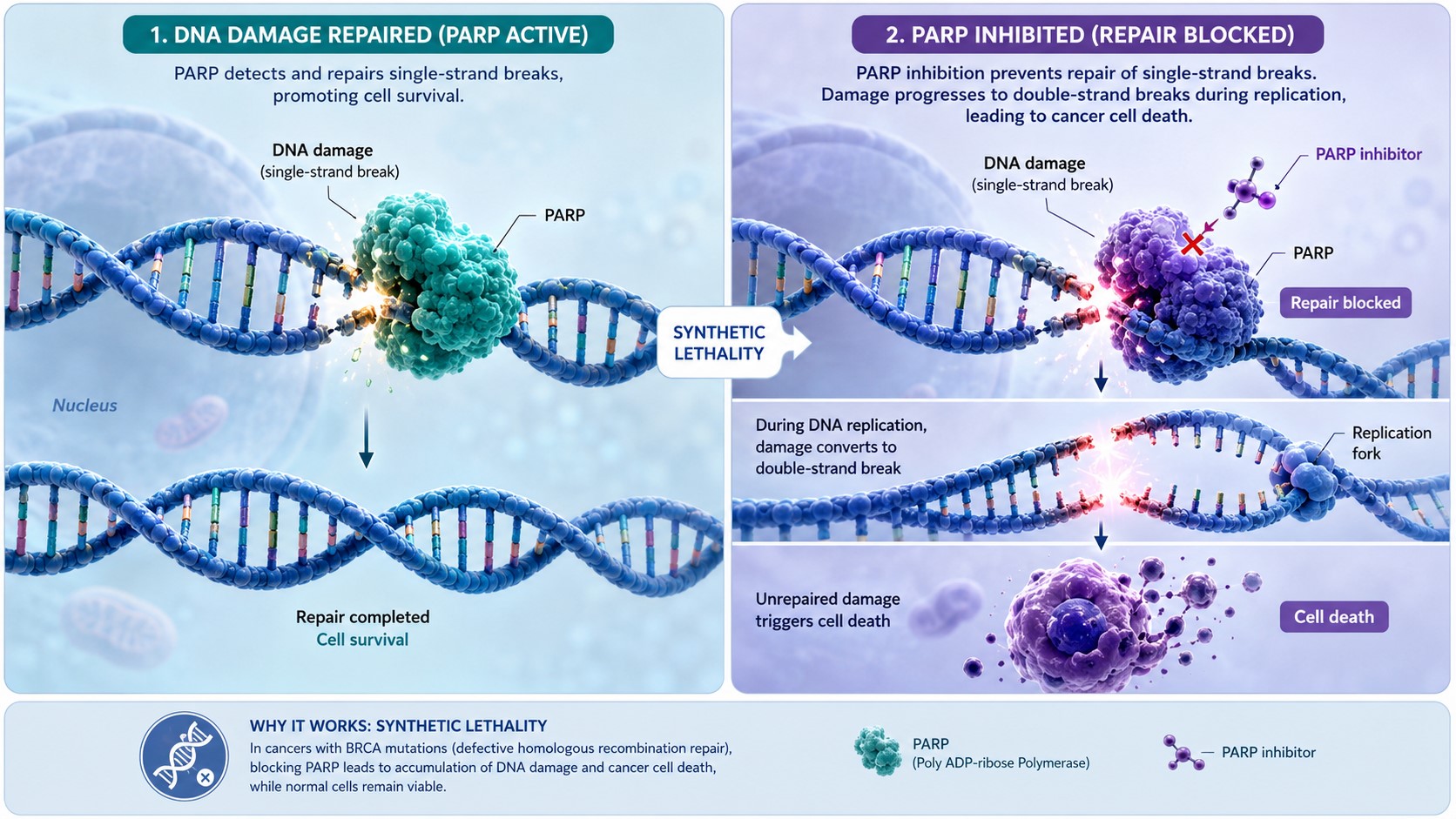
Every cell in the body accumulates DNA damage daily. PARP – which stands for Poly (ADP-ribose) Polymerase – is an enzyme that detects single-strand DNA breaks and triggers their repair. Think of it as a cellular alarm system that spots small cracks in the DNA ladder and calls in the repair crew.
Cancer cells, like all cells, depend on this system to survive. In normal cells, there are multiple backup repair pathways. But in certain cancer cells – particularly those with mutations in the BRCA1 or BRCA2 genes – one of those backup systems (homologous recombination) is already broken.
How PARP Inhibitors Exploit Cancer Cell Weakness — Synthetic Lethality
When a PARP inhibitor blocks PARP from working, single-strand DNA breaks accumulate and convert into double-strand breaks. In a healthy cell, the homologous recombination pathway fixes this. But in a BRCA-mutated cancer cell, that backup pathway is gone.
The result: the cancer cell cannot repair its DNA and dies.
This is called synthetic lethality – two molecular deficiencies that are individually survivable but lethal together. It is the scientific principle behind why PARP inhibitors work so powerfully in BRCA-mutated cancers, while still offering some benefit in cancers with other homologous recombination deficiencies (HRD).
Quick Overview — Olaparib, Niraparib, and Rucaparib at a Glance
| Feature | Olaparib (Lynparza) | Niraparib (Zejula) | Rucaparib (Rubraca) |
|---|---|---|---|
| Manufacturer | AstraZeneca / MSD | GSK | Clovis Oncology |
| FDA First Approval | 2014 | 2017 | 2016 |
| Approved Cancer Types | Ovarian, breast, prostate, pancreatic | Ovarian | Ovarian (prostate withdrawn 2022) |
| Requires BRCA/HRD Testing? | Yes (for most indications) | No (ovarian maintenance) | Yes |
| Dosing | 300 mg twice daily | 200–300 mg once daily | 600 mg twice daily |
| Key Trials | SOLO-1, OlympiAD, PROfound | PRIMA, NOVA | ARIEL3, TRITON2 |
Olaparib (Lynparza) — Key Facts
Olaparib was the first PARP inhibitor to receive FDA approval, in December 2014. It is a tablet taken twice daily and has the broadest approval of the three drugs discussed here.
It works best in patients with confirmed BRCA1 or BRCA2 mutations, though some approvals extend to patients with HRD-positive tumors without a BRCA mutation.
Approved indications include:
- Ovarian cancer (first-line maintenance and relapsed disease)
- HER2-negative metastatic breast cancer with germline BRCA mutation
- Metastatic castration-resistant prostate cancer with BRCA or HRR gene mutations
- Metastatic pancreatic cancer with germline BRCA mutation
Niraparib (Zejula) — Key Facts
Niraparib is a once-daily capsule approved in 2017. Its most important clinical distinction is that it is approved for first-line maintenance therapy in advanced ovarian cancer regardless of BRCA or HRD status – making it the most accessible PARP inhibitor in terms of patient selection.
This means an oncologist does not have to wait for biomarker test results to initiate maintenance therapy with niraparib in an eligible ovarian cancer patient.
Approved indications include:
- First-line maintenance therapy in advanced ovarian, fallopian tube, or primary peritoneal cancer (all-comers after platinum response)
- Maintenance of recurrent ovarian cancer (platinum-sensitive)
Rucaparib (Rubraca) — Key Facts
Rucaparib received accelerated FDA approval in 2016 for BRCA-mutated ovarian cancer. It was also approved for prostate cancer but that indication was voluntarily withdrawn by Clovis Oncology in 2022 following trial results showing it did not improve overall survival compared to newer hormonal therapies in a broader patient population.
Its current approved use is limited to recurrent ovarian cancer with BRCA mutations after two or more prior chemotherapy regimens.
Approved indications include:
- Recurrent BRCA-mutated ovarian, fallopian tube, or primary peritoneal cancer (maintenance and treatment)
Approved Indications — What Is Each Drug Used For?
Olaparib Indications
Olaparib’s breadth of approval is unmatched among PARP inhibitors. Key approvals include:
- Ovarian cancer (first-line maintenance): For patients with BRCA-mutated advanced ovarian cancer who responded to platinum-based chemotherapy – the SOLO-1 trial showed a significant progression-free survival benefit.
- Breast cancer: For patients with HER2-negative metastatic breast cancer and a germline BRCA mutation – the OlympiAD trial demonstrated improved progression-free survival over chemotherapy.
- Prostate cancer: For metastatic castration-resistant prostate cancer with BRCA1/2 or other HRR mutations – shown in the PROfound trial.
- Pancreatic cancer: Maintenance therapy for metastatic pancreatic cancer with germline BRCA mutation following platinum-based chemotherapy.
Niraparib Indications
Niraparib’s strength lies in ovarian cancer maintenance therapy. The PRIMA trial established it as the first PARP inhibitor approved for all-comer first-line ovarian cancer maintenance – including patients without BRCA mutations or HRD – though the benefit was most pronounced in HRD-positive patients.
Rucaparib Indications
Rucaparib’s current role is narrower. It remains an option for recurrent BRCA-mutated ovarian cancer in patients who have received at least two prior chemotherapy regimens. Oncologists today typically consider olaparib or niraparib first given their broader trial data and established safety profiles.
Efficacy Comparison — How Well Do They Work?
Clinical Trial Results Summary
Each PARP inhibitor has been studied in landmark phase 3 trials that define when and for whom these drugs provide meaningful benefit.
SOLO-1 (Olaparib): In patients with newly diagnosed BRCA-mutated advanced ovarian cancer who responded to platinum chemotherapy, olaparib maintenance therapy resulted in a median progression-free survival of 56 months versus 13.8 months with placebo — a landmark result that established PARP inhibitors as standard first-line maintenance in BRCA-mutated ovarian cancer.
PRIMA (Niraparib): In all patients with newly diagnosed advanced ovarian cancer after platinum response, niraparib improved progression-free survival in the overall population (13.8 vs 8.2 months). The benefit was more pronounced in the HRD-positive subgroup (21.9 vs 10.4 months), but a statistically significant – if more modest – improvement was also seen in HRD-negative patients.
ARIEL3 (Rucaparib): In platinum-sensitive recurrent ovarian cancer, rucaparib maintenance showed significant progression-free survival improvement across BRCA-mutated, HRD-positive, and intent-to-treat populations. The BRCA-mutated subgroup had the strongest benefit (16.6 vs 5.4 months).
Progression-Free Survival — What the Numbers Mean for Patients
Progression-free survival (PFS) is the time a patient lives without the cancer growing or spreading. It is the primary endpoint in most PARP inhibitor trials.
All three drugs have demonstrated meaningful PFS benefits compared to placebo in their respective approved populations. However, overall survival data are more complex – longer follow-up and the impact of subsequent treatments after progression make OS data harder to interpret cleanly for these agents.
BRCA-Mutated vs HRD-Positive vs All-Comers
The clearest benefit from all three PARP inhibitors is seen in patients with BRCA1 or BRCA2 mutations. The benefit gradually diminishes as the biomarker requirement is relaxed:
- BRCA-mutated → strongest benefit
- HRD-positive (includes BRCA-mutated and HRD without BRCA) → moderate-to-strong benefit
- All-comers (HRD-negative included) → benefit exists but is smaller
Niraparib is the only drug with first-line approval for all-comers. Olaparib and rucaparib require BRCA or HRD testing.

Side Effects and Safety Profile
All PARP inhibitors share a class-related side effect profile, but differ in certain specifics that matter for individual patients.
Common Side Effects of Olaparib
- Nausea (most common, often manageable with antiemetics)
- Fatigue
- Anemia
- Vomiting
- Diarrhea
- Decreased appetite
Olaparib’s twice-daily dosing can be adjusted to 250 mg twice daily for patients experiencing significant toxicity.
Common Side Effects of Niraparib
- Thrombocytopenia (low platelet count) – more prominent with niraparib than with olaparib or rucaparib; dose adjustments based on body weight and platelet count at baseline have significantly reduced this risk in clinical practice
- Nausea
- Anemia
- Fatigue
- Hypertension – a notable cardiovascular side effect requiring monitoring
- Constipation
Niraparib is now initiated at an individualized starting dose (200 mg/day for patients under 77 kg or with platelet count below 150,000/µL; 300 mg/day for others), which has improved tolerability significantly.
Common Side Effects of Rucaparib
- Nausea and vomiting (among the most common)
- Fatigue
- Anemia
- Elevated liver enzymes (AST/ALT) – more frequently reported with rucaparib than with the other two
- Photosensitivity
Serious Risks Shared by All Three: MDS and Pneumonitis
A rare but serious complication of PARP inhibitor therapy is myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML) – conditions in which the bone marrow fails to produce normal blood cells. The risk is low (approximately 1–2%) but requires monitoring. If MDS or AML is confirmed, the PARP inhibitor must be discontinued.
Pneumonitis (lung inflammation) has also been reported across all three agents. Patients who develop new or worsening respiratory symptoms should be evaluated promptly.
How Oncologists Choose Between These Three Drugs
When an oncologist selects a PARP inhibitor, it is rarely arbitrary. The decision depends on several patient- and disease-specific factors.
Patient’s BRCA/HRD Status
This is often the first filter. If a patient has a confirmed BRCA1 or BRCA2 mutation, all three drugs are potentially relevant, but olaparib has the deepest evidence base and broadest indications. If a patient is BRCA-negative but HRD-positive, olaparib and niraparib both have approvals covering this group. If biomarker testing is unavailable or the patient is HRD-negative, niraparib is the only first-line option with data supporting use in that context.
Cancer Type and Line of Treatment
- Ovarian cancer, first-line maintenance: Olaparib (BRCA-mutated) or niraparib (all-comers or HRD-positive) are the standard choices.
- Breast cancer: Olaparib is the only approved PARP inhibitor.
- Prostate cancer: Olaparib is the primary option following rucaparib’s withdrawal.
- Pancreatic cancer: Olaparib is the only approved PARP inhibitor.
- Recurrent ovarian cancer (second-line or later): All three have data; olaparib and niraparib have stronger current positioning.
Tolerability and Patient-Specific Factors
Niraparib’s thrombocytopenia risk and hypertension signal make it a more cautious choice in patients with pre-existing low platelet counts or uncontrolled hypertension. Rucaparib’s liver enzyme elevations warrant caution in patients with underlying hepatic issues. Olaparib’s nausea is generally well-managed but can be a quality-of-life concern.
Dosing convenience also matters: niraparib’s once-daily schedule may improve adherence compared to olaparib’s and rucaparib’s twice-daily regimens.
Drug Availability and Cost
In many countries – including low- and middle-income settings – access to these drugs depends on local regulatory approvals, formulary listings, and financial assistance programs. In Bangladesh and similar markets, availability may differ from what is reflected in FDA or EMA approvals. Patients should check with their oncologist and pharmacist about what is locally available.
For updated drug availability and guidance, visit Medicine for World.
Dosing and Administration
| Drug | Dose | Schedule | Food Requirement |
|---|---|---|---|
| Olaparib (Lynparza) | 300 mg | Twice daily | With or without food |
| Niraparib (Zejula) | 200–300 mg (individualized) | Once daily | With or without food |
| Rucaparib (Rubraca) | 600 mg | Twice daily | With or without food |
Olaparib Dosing
The standard dose is 300 mg taken orally twice daily. For patients who cannot tolerate this dose, a reduction to 250 mg twice daily is available. Olaparib tablets should not be crushed or dissolved.
Niraparib Dosing
Niraparib’s starting dose is individualized based on body weight and baseline platelet count. Patients weighing less than 77 kg or with a platelet count below 150,000/µL begin at 200 mg once daily. Others start at 300 mg once daily. This individualized approach was introduced following evidence that it significantly reduces grade 3 or higher hematologic toxicity.
Rucaparib Dosing
The standard dose is 600 mg taken orally twice daily. Dose reductions are available for toxicity management.
Common Mistakes Patients and Caregivers Make
1. Assuming all PARP inhibitors are interchangeable. They are not. Each has specific approved indications. A patient with breast cancer cannot simply substitute niraparib for olaparib – only olaparib is approved for that setting.
2. Stopping the medication when side effects appear without telling the oncologist. Most PARP inhibitor side effects can be managed with dose adjustments, antiemetics, or supportive care. Stopping abruptly without medical guidance may compromise treatment outcomes.
3. Not getting BRCA/HRD testing before discussing options. Knowing your biomarker status opens up or closes off specific drug options. Testing should be done before, or as early as possible in, the treatment course.
4. Overlooking drug interactions. PARP inhibitors are metabolized through the CYP3A4 enzyme pathway. Concurrent use of strong CYP3A4 inhibitors (like certain antifungals or antibiotics) or inducers (like rifampicin or St. John’s Wort) can significantly alter drug levels. Always review all medications with the treating team.
5. Assuming rucaparib is still as widely available as it was. Clovis Oncology’s voluntary withdrawal of rucaparib’s prostate cancer indication in 2022 and its subsequent limited presence in the market means patients and caregivers should verify current availability and guidelines with their care team.
Frequently Asked Questions (FAQs)
Q1: What is the difference between Olaparib, Niraparib, and Rucaparib?
All three are PARP inhibitors that block the PARP enzyme, preventing cancer cells from repairing damaged DNA. The key differences lie in their approved indications, dosing schedules, biomarker requirements, and side effect profiles. Olaparib has the broadest approvals across multiple cancer types. Niraparib is the only one approved for first-line ovarian cancer maintenance in patients regardless of BRCA/HRD status. Rucaparib has a narrower current role, primarily in BRCA-mutated recurrent ovarian cancer.
Q2: Which PARP inhibitor is used for BRCA-mutated ovarian cancer?
All three have been studied and approved for BRCA-mutated ovarian cancer in various settings. Olaparib (SOLO-1 trial) and niraparib (PRIMA trial) are the preferred first-line maintenance options. Rucaparib (ARIEL3 trial) is an option for later lines of therapy in BRCA-mutated patients.
Q3: Can PARP inhibitors be used without a BRCA mutation?
Yes. Niraparib is the most relevant example – it is approved for first-line ovarian cancer maintenance regardless of BRCA or HRD status, though benefit is most pronounced in HRD-positive patients. Olaparib also has HRD-positive approvals beyond strict BRCA selection in some settings.
Q4: What are the most common side effects of PARP inhibitors?
The class-wide side effects include nausea, fatigue, anemia, and decreased appetite. Niraparib carries a more notable risk of thrombocytopenia (low platelets) and hypertension. Rucaparib is more associated with liver enzyme elevations. All three carry a small but real risk of myelodysplastic syndrome (MDS) with long-term use.
Q5: Is Rucaparib still available and FDA-approved?
Rucaparib’s prostate cancer indication was voluntarily withdrawn by Clovis Oncology in June 2022 after the TRITON3 trial showed no overall survival benefit in a broader population. As of the time of this writing, rucaparib (Rubraca) retains approval for recurrent BRCA-mutated ovarian cancer, but clinicians should verify the latest regulatory status with authoritative sources such as the FDA website or NCCN guidelines, as the drug’s commercial availability has become limited.
Conclusion — Which PARP Inhibitor Should You Consider?
There is no universal answer to which PARP inhibitor is “best.” The right choice depends on the specific cancer type, the patient’s biomarker status, the line of treatment, and the patient’s overall health profile.
As a general framework:
- If the patient has BRCA-mutated ovarian, breast, prostate, or pancreatic cancer, olaparib should be the first conversation.
- If the patient has newly diagnosed advanced ovarian cancer and BRCA/HRD status is unknown or negative, niraparib’s all-comer approval makes it an important option.
- If the patient is in a later line of treatment for BRCA-mutated ovarian cancer, all three have historical data, but olaparib and niraparib have stronger current positioning.
What matters most is that every patient has this conversation with their oncologist – ideally one who specializes in gynecologic or relevant cancer oncology – before any treatment decision is made.
For more oncology drug guides, treatment overviews, and patient-friendly medical information, visit Medicine for World.
References and Further Reading
- FDA Drug Label: Olaparib (Lynparza) — fda.gov
- FDA Drug Label: Niraparib (Zejula) — fda.gov
- FDA Drug Label: Rucaparib (Rubraca) — fda.gov
- Moore K, et al. “Olaparib Maintenance Therapy in Newly Diagnosed Advanced Ovarian Cancer.” NEJM, 2018 (SOLO-1 trial)
- González-Martín A, et al. “Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer.” NEJM, 2019 (PRIMA trial)
- Coleman RL, et al. “Rucaparib Maintenance Treatment for Recurrent Ovarian Carcinoma.” Lancet, 2017 (ARIEL3 trial)
- NCCN Clinical Practice Guidelines in Oncology: Ovarian Cancer — nccn.org
- NCCN Clinical Practice Guidelines in Oncology: Breast Cancer — nccn.org
This article was prepared by the editorial team at Medicine for World for informational and educational purposes. It does not replace professional medical advice. Always consult a qualified oncologist or pharmacist for guidance specific to your clinical situation.
Last updated: June 2026 | Published on mfw.com.bd